Lecture Notes, Biology 203, Human Sexuality and Reproduction
Sexually Transmitted Diseases
- Introduction
- Diseases, organization
- More serious, life threatening: AIDS, syphilis
- Serious consequences: gonorrhea, chlamydia, herpes, genital warts
- Less serious: trichomonas, candida, gardnerella
- Characteristics of diseases: cause, how you get it, symptoms and incubation period, complications, long-term risk, diagnosis, treatment, vaccine, epidemiology, misc. issues
- Center for Disease Control, Atlanta: records case frequency, distribution for reportable diseases, traces contacts, epidemiology
- Worldwide STD cases (graph)
- Most common: Trichomonas
- Middle group: chlamydia, gonorrhea, genital warts, genital herpes
- Least common: AIDS
- Responsibility/ethics: the person who has the symptoms of an STD has the responsibility to tell their sexual partners about an STD
- Acquired Immune Deficiency Syndrome (AIDS)
- Incidence/mortality
- 1985: 1200 cases/450 dead
- 1997: 600,000 cases/380,000 dead
- 6/2001: 793,000 cases/458,000 dead (649,000 male, 135,000 female, 9000 children)
- 5th leading cause of death in U.S. for ages 25-44
- In top 10, Illinois 6th highest state, Chicago 6th highest city (St. Louis and MO not in top 10)
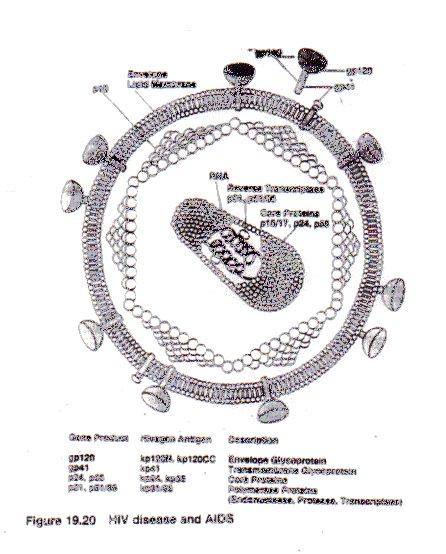
- Infectious agent: human immunodeficiency virus (HIV)
- Viruses can't reproduce by themselves, but require a host cell to supply the energy and other materials necessary
- A virus binds to a specific host cell by attaching to receptor molecules on the host cell surface.
- A host cell with no receptors for a particular virus can't be infected by that virus.
- The receptor on human cells that binds HIV is a molecule called CD4, found on immune system cells, as well as on cells in the brain and intestinal lining
- Cells of the immune system (T-helper lymphocytes) that are CD4-positive are ones that help make a protective response to infectious agents (such as bacteria, viruses, fungi, protozoa)
- HIV are made of RNA (containing genetic information) surrounded by viral coat proteins and enclosed in a viral envelope (membrane material acquired when the virus left the preceding host cell)
- Viral proteins in the envelope are recognized by the human immune system, but the immune response is not protective.
- Another viral protein, fusin, helps the virus enter the host cell
- HIV binds to CD4-positive lymphocytes and eventually destroys them, increasing the infected person's susceptibility to infectious diseases
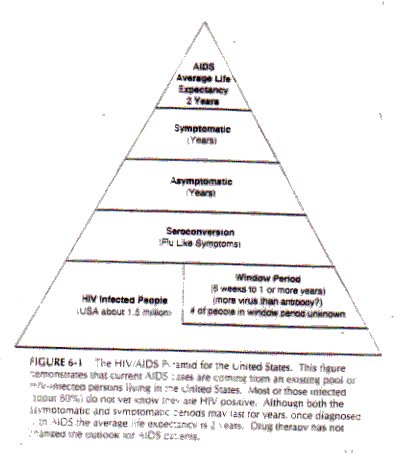
- Many more people are infected with HIV than have HIV disease or AIDS (see diagram)
- The largest number of people are infected with the virus, but have no symptoms.
- After 6 weeks to 4 months, these people will develop anti-HIV antibodies--these are detected in AIDS screening tests.
- Eventually, people infected with the virus begin to have symptoms associated with viral infection.
- After 2 to 10 years, most people will have developed AIDS, the most serious form of HIV disease
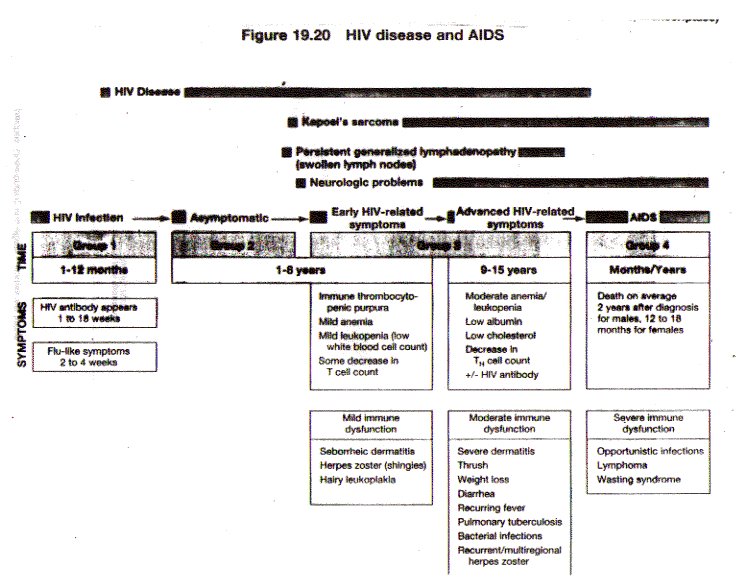
- See timeline handout (paper or online) for progressive appearance of symptoms
- Phase/stages of HIV infection
- HIV enters body
- HIV binds to cells via CD4 receptors
- Infected cell begins to make more virus slowly
- No symptoms at this stage, no anti-HIV antibody, but virus is present
- After few weeks, immune system makes anti-HIV antibodies that can be detected by the AIDS screening test as soon as enough is present
- People remain asymptomatic for years, producing both anti-HIV antibody and HIV virus
- Eventually people begin to display symptoms (early HIV disease--clotting defects, decreased numbers of red and white blood cells
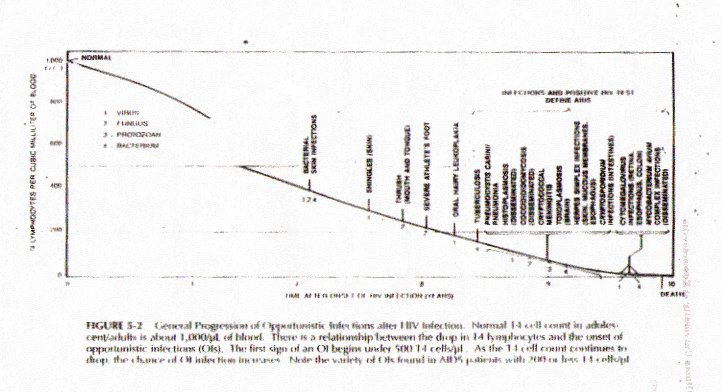
- Later, maybe as long as 9 to 15 years later, people display symptoms of more advance HIV disease (some opportunistic infections, reduction in helper-T lymphocyte numbers)
- As T lymphocyte numbers are reduced, susceptibility to infectious diseases increases, and eventually the person has fully developed AIDS
- See paper or online handout
- Symptoms and signs of HIV disease and AIDS
- Symptoms: weakness, fatigue, night sweats, fever, swollen lymph nodes, diarrhea, weight loss
- Neurological signs: memory loss, loss of coordination, depression, paralysis, possibly leading to death
- Opportunistic infections: systemic fungal infections, unusual Pneumocystis pneumonia, tuberculosis, etc.
- Rare form of skin cancer: Kaposi's sarcoma (not seen in all AIDS patients)
- Progression from HIV infection to AIDS
| Time from infection with HIV |
Percent who will have AIDS |
| 3 years |
4% |
| 5 years |
14% |
| 6 years |
27% |
| 7 years |
34% |
| 9 years |
42% |
| 10 years |
50% |
- About 75% of AIDS patients die within 2 years after diagnosis (with fully developed AIDS)
- As of 6/2001, the CDC Surveillance Report on AIDS reported that
- Worldwide, there were 40 million people infected with HIV disease
- Worldwide, in 2001, 3 million people died of AIDS, including 1.1 million women and 580,000 children
- Worldwide, 48% of adult cases are in women
- 95% of adults with AIDS and 90% of new cases live in the developing world
- In the USA, in men, 50% of cases are attributable to male-to-male transmission, 23% are IV drug users
- In the USA, in women, 40% of cases are attributable to contact with infected men, and 27% are IV drug users
- Between 1996 and 1997, deaths from AIDS declined by 12%, probably due to better treatments now available
- HIV transmission
- Virus enters body through linings of vagina, rectum, urethra, mouth or openings in skin
- Body fluids that contain sufficient amounts of virus to infect another person: blood, semen, vaginal fluids, breast milk, colostrum (but not tears, saliva, or urine)
- Routes of infection
- Mother to fetus/newborn (HIV crosses placenta to cause intrauterine infection, or is transmitted during birth or breast feeding)
- Sexual intercourse (vaginal, rectal, or oral, with the receiving partner most at risk)
- Contact with blood, semen, or vaginal fluids (needles, sex, razors....)
- HIV is not transferred by casual contact at home or work, coughing or sneezing, sharing drinking glasses, kissing, biting or spitting unless blood is transferred, mosquitos, tears, using saunas/hot tubs, visiting spas or health clubs
- From lowest risk to highest (most likely to transmit HIV): abstinence, oral sex, vaginal sex with latex condom and foam, anal sex with latex condom, unprotected anal sex (receiving partner)
- What inactivates HIV? (drying (99% in 3 days), bleach, 70% ethanol, Lysol, hydrogen peroxide)
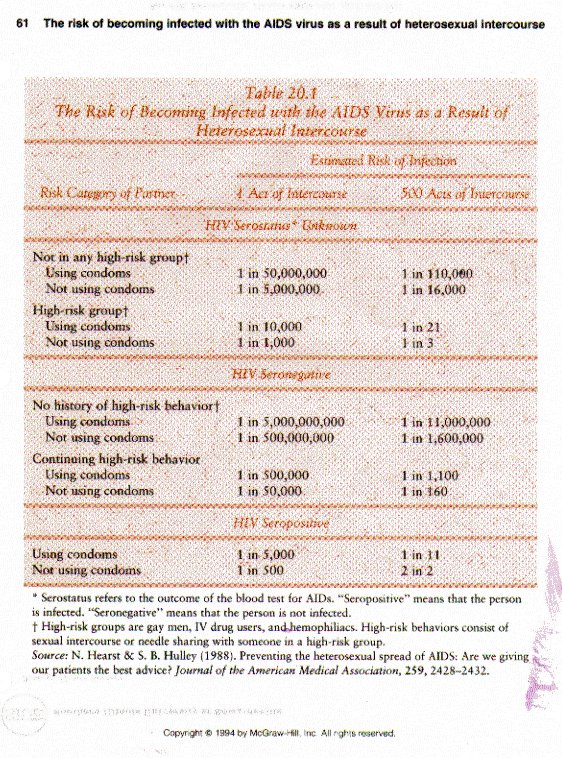
- See paper and online handout on chance of transmission of HIV after 1 or 500 acts of intercourse under various circumstances
- HIV vaccine?
- External and internal viral proteins in conventional vaccine have not provided protection from HIV infection
- Fusin protein might be useful in a vaccine
- Genetic "vaccines" may be useful eventually
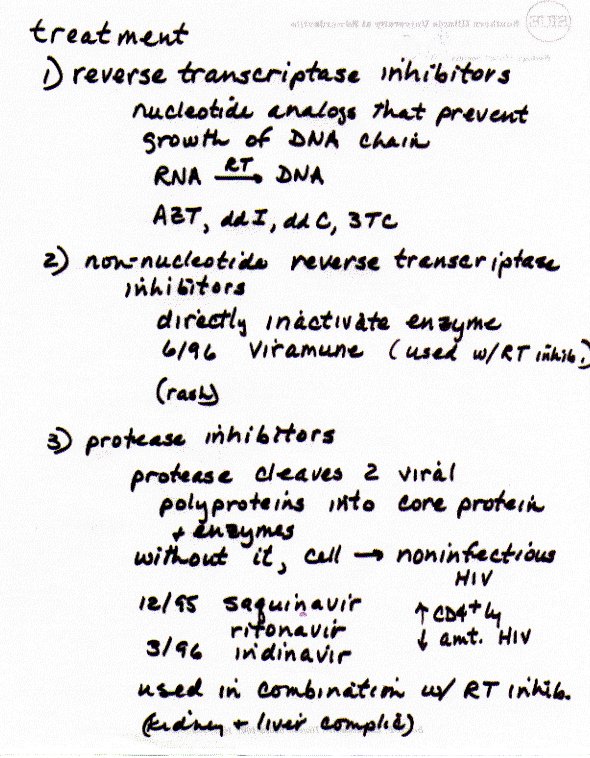
- Treatments
- Most treatments block reverse transcriptase, a viral enzyme that converts viral RNA to DNA, necessary to use host cell's apparatus for making proteins
- Newer drugs decrease viral load by up to 70%, prolong life of AIDS patients, increase % of CD4-positive cells
- Combinations of drugs decrease the chance that patients will become resistant compared to use of a single drug
- Nucleotide reverse transcriptase inhibitors: prevent growth of DNA chain being synthesized from viral RNA (AZT, ddI, ddC, 3TC)
- Non-nucleotide reverse transcriptase inhibitors (directly inactivate RT enzyme, often used with nucl. RT inhibitor)
- Protease inhibitors (block action of a viral enzyme that cleaves larger inactive viral proteins into smaller active proteins--without protease, host cell produces noninfectious HIV, often combined with RT inhibitors)
- Complications and side effects include rashes, kidney and liver damage, drug resistance
- Syphilis
- Picture of spirochete bacteria that cause syphilis (Treponema pallidum)
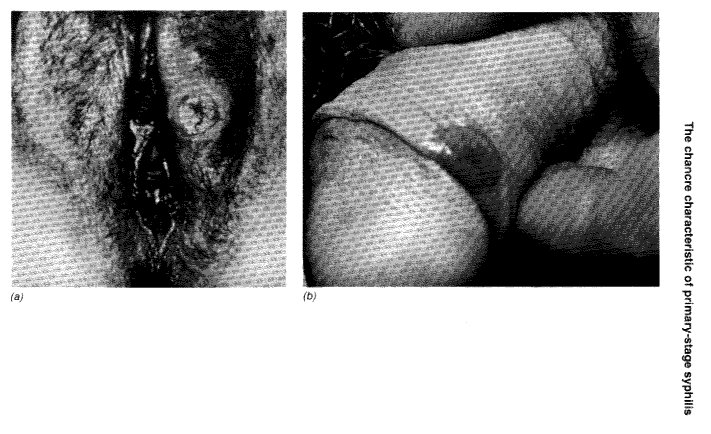
- Picture of primary syphilitic lesions, or chancres, male (right) and female (left)
- Three stages of syphilis
- Primary syphilis
- Three week incubation period between exposure and appearance of lesion (chancre)
- Chancre may be internal or external, is painless, and goes away in 2-6 weeks without treatment
- Fluid from chancre is infectious (contains bacteria)
- Can diagnose by using special microscopic technique to look at the bacteria (blood test not useful)
- Bacteria transferred to another person by direct sexual contact (contact with fluid from lesion)
- Person may be asymptomatic for 2-24 weeks before next stage
- Secondary syphilis
- Skin rash typical of secondary syphilis
- Rash is systemic, may occur on thighs or trunk, with many lesions
- Secondary syphilis is contagious, but treatable
- Rash goes away in 2-6 weeks regardless of treatment
- Blood test for anti-bacterial antibodies useful in diagnosis during secondary stage
- Person may be asymptomatic for 3 to 30 years or more after secondary stage
- Tertiary syphilis
- 50% of stage 2 never develop tertiary stage (or die of something else first)
- 25% develop serious tertiary stage symptoms
- 25% develop less serious symptoms
- Bacteria no longer detectable in tertiary syphilis
- Immune response made to bacteria causes damage to small blood vessels in various organs (brain, heart, kidney, liver, eyes, skin, bone)
- Symptoms depend on organ damaged
- Not treatable, not contagious, damage not reversible
- Blood test for antibacterial antibodies useful in diagnosis
- Table comparing stages of syphilis
| Stage
|
Blood test useful?
|
Contagious?
|
Treatable?
|
| 1
|
No
|
Yes
|
Yes
|
| 2
|
Yes (VDRL)
|
Yes
|
Yes
|
| 3
|
Yes (VDRL)
|
No
|
No
|
- In 1999, St. Louis was 8th and Chicago 12th in case frequency of syphilis in large cities
- Men (peak ages 35-39) are 50% more likely than women (peak ages 20-29) to have syphilis
- Black Americans are 30X more likely to have syphilis that white Americans
- After a peak in case frequency in 1991, incidence of syphilis has declined over 80% in US, and is now at the lowest frequency since 1941
- More than 50% of women pass through stages 1 and 2 without knowing it
- Treatment: penicillin (100% curable in stages 1 and 2, within 2-3 days not contagious, but must complete treatment)
- Congenital syphilis
- 100% preventable if mother diagnosed and treated before 16th week of pregnancy
- Bacteria can cross placenta to infect fetus before birth
- Baby is born with stage 2 syphilis
- 25% of infected fetuses die before birth, 25% die after birth, 25% born with stage 2 syphilis, and 25% not infected
- Case frequency of congenital syphilis closely follows frequency in pregnant women--both have been declining since 1991
- Gonorrhea and Chlamydia (both caused by bacteria, often found in mixed infections)
- Gonorrhea
- Caused by small round bacteria often found in pairs, Neisseria gonorrhoeae
- 90% of women and 10% of men are asymptomatic
- Highly contagious
- Spreads rapidly through sexually active population
- In 1999, St. Louis was 3rd and Chicago 14th in case frequency of gonorrhea in large cities
- Transferred by direct sexual contact with infectious discharge
- Short incubation period--3 to 5 days
- Can be genital, anal/rectal, oral, or eye infection
- In men, it is most commonly a urethral infection; in women, cervical or urethral
- Symptoms in men: urethral discharge, burning urination, cloudy urine
- Symptoms in women (if any): inflammation of cervix, thick, yellowish discharge, possibly burning urination, cloudy urine
- Usually remains a local infection, causing little permanent damage
- If untreated in women, sometimes causes pelvic inflammatory disease (PID), which may lead to sterility
- If disease becomes systemic (moves away from reproductive tract), may move into blood, then joints, heart, liver
- Diagnosis
- Microscopic observation of discharge--should see white blood cells with bacteria inside (50% accurate)
- Observation of characteristics of discharge
- May grow and test bacteria in culture (slow)
- May use fluorescent antibody test to identify bacteria
- Treatment
- Penicillin (or other antibiotics if person is allergic to penicillin)
- Complete the treatment, usually if no symptoms and another culture is negative, after 3-7 days safe to resume having sex
- If symptoms don't go away, bacteria may be resistant to penicillin or other drug--try another antibiotic
- Could also be a mixed infection with both gonorrhea and chlamydia (chlamydia not affected by penicillin)
- Special cautions for women
- Women who are sexually active, especially with more than one partner, should have cultures done every three months
- Half of women who have gonorrhea also have chlamydia
- Half of women who have untreated gonorrhea develop PID
- Women should have a culture done before an IUD is inserted
- Special cautions for pregnant women
- Newborns are treated with silver nitrate to prevent gonococcal ophthalmia, an eye infection that can lead to blindness
- 1/3 of women who have gonorrhea also have streptococcus B infections, which can be dangerous for newborns
- Special cautions for men
- Female sexual partners may be asymptomatic, but infected and infectious
- Men who continue to have symptoms after treatment may have postgonococcal urethritis (PGU)--80% is caused by chlamydia
- 30% of men who have gonorrhea also have chlamydia
- Chlamydia
- Caused by bacteria called Chlamydia trachomatis
- In men, causes postgonococcal urethritis, nongonococcal urethritis, nonspecific urethritis
- In women, causes postgonococcal cervicitis
- Differences from gonorrhea
- Different susceptibility to antibiotics (not susceptible to penicillin)
- Longer incubation period (3 weeks)
- Spreads more slowly through a population
- Milder symptoms
- More likely to cause scarring leading to infertility as a result of PID
- 50-90% of PID is caused by chlamydia
- Pregnant women who have an active chlamydia infection at the time of delivery may infect the newborn baby, leading to eye infections that can cause blindness or respiratory tract infections (pneumonia)
- Complications: sterility due to PID or epididymitis, occasionally becomes systemic
- In women, cervical infection may move into uterus and Fallopian tubes
- In men, urethral infection may move into the epididymis
- Transfered by direct sexual contact
- Symptoms (often asymptomatic, milder than gonorrhea)
- Women: slight vaginal discharge, painful intercourse, fever, lower abdominal pain
- Men: urethral discharge, burning urination
- Diagnosis
- Slow, difficult to grow in culture
- Can use fluorescent antibody test, which is faster
- Treatment
- Tetracycline or sulfa drugs, for three weeks
- Must treat both partners, disease "ping-pongs" between them
- Well when there are no symptoms and treatment is completed
- Genital Herpes and Genital Warts (both viral, both linked to cervical cancer)
- Genital herpes (caused by HSV-1 and HSV-2, members of large herpes virus family)
- Either HSV-1 or HSV-2 may cause either oral or genital herpes
- No cure--virus becomes latent in spinal cord nerves between outbreaks
- Virus moves along peripheral nerves to surface of skin or mucous membranes during recurrent outbreaks
- During active outbreak, lesions produce infectious fluid containing virus
- After lesions have healed, little virus is shed
- Virus remains hidden in nerves until next outbreak
- Interval between outbreaks may be 1 month to 6 or 12 months
- More frequent outbreaks early in infections, less frequent later on
- Outbreaks may be triggered by emotional stress, sunburn, fever, local irritation, pregnancy, menstruation, birth control pills
- Some people experience a prodrome 6 hrs. to 2 days before an outbreak--feel tingling, pain near where lesions will appear
- Pictures of herpes lesions in female and male
- Symptoms
- Group or cluster of small blisterlike lesions
- Lesions may be itchy or painful
- Painfully swollen lymph nodes draining site of lesions (often groin nodes)
- Open lesions produce virus-containing fluid
- Heal in 3 to 10 days
- Once healed, shed virus in small quantities for few more days
- Diagnosis
- Inspection of active lesions
- Culture virus in host cells
- Fluorescent antibody testing
- Treatment
- Acyclovir and other antiviral drugs now available
- Drugs more effective in first outbreak, which is often the most severe
- Improve symptoms and shorten outbreak
- Keep lesions clean and dry, to decrease chance of secondary bacterial infection
- Placebo effect (if people think that a particular treatment will help, sometimes it will, even if there is no biological reason for it to help)
- Complications and cautions
- Infection of eyes (herpetic keratosis)
- In immunocompromised person, may become systemic and possibly lethal (AIDS patients, infants, elderly, malnourished, cancer patients)
- Women who have recurrent HSV-2 infections have a 5-10% greater risk of cervical cancer
- Pregnant women who have an outbreak near (within 4 weeks of) delivery should have Caesarian section delivery to avoid infections during vaginal birth
- Of babies born to women with recent genital outbreak, 50% are not infected, 30% die, 10% are blind or brain-damaged, 10% are infected, but have no serious problems
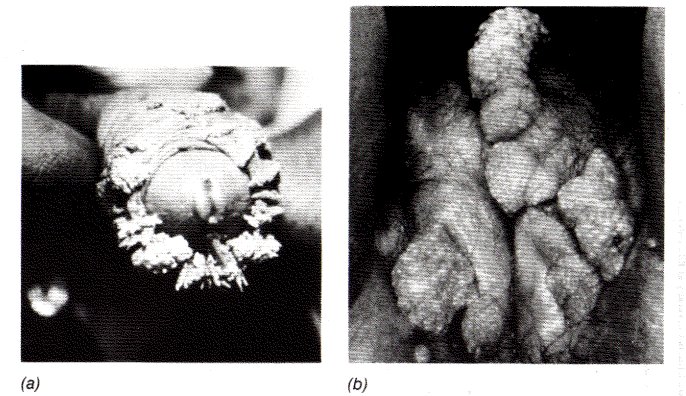
- Genital warts (condyloma)
- Caused by human papilloma virus (over 30 types) (HPV, a member of a large family of related viruses)
- Persistent cervical infection in women can lead to cervical cancer (virus type 16 most commonly, also 18, 31, 45)
- Also associated with anal cancer in both men (especially men who have sex with men and HIV-infected men) and women, and with penile cancer in men
- Pap smear can be used to diagnose cervical or anal cancer
- 60-85% of sexual partners of those infected also are infected
- Transferred by vaginal, oral, or anal sex
- People who have multiple sexual partners, other STD's or impaired resistance to infection are especially at risk
- Long incubation period--2 to 3 months
- First appear as cluster of tiny growths
- Later, if not treated, may grow into much larger warts (picture)
- Warts may itch, bleed, or have no symptoms
- Warts may be small or large, internal (often flattened) or external (white vinegar can make them more visible)
- Treatment
- Antibiotics not useful in treating viral infections
- May treat with drugs that kill human host cells
- May freeze or burn off warts
- If virus is still present, warts may regrow and require re-treatment
- If untreated, some HPV cause the development of precancerous cells in a Pap smear or cervical cancer
- Avoid sex until warts are treated and healed
- Statistics
- Affects 15% of population between the ages of 15 and 49 (20 million in U.S.)
- Most common STD in younger people--43% of female college students infected at some time during one three year period, 14% new cases each year of the study
- New cases each year: 5.5 million
- Case frequencies in men are similar to those in women
- Candida, Trichomonas, Gardnerella (less serious diseases, with no long term risks)
- Candida
- Also called yeast infection, monilia--caused by the fungus Candida albicans
- Yeast may be part of the normal flora of the vagina (organisms normally present in or on your body all the time)
- In vaginal ecology, there is a mixed population of microorganisms that keep each other in balance and produce the normally acidic conditions
- Disturbance of this ecosystem creates an imbalance in the microbial populations that may lead to overgrowth of one type of microorganism
- A change in hormone production (pregnancy, menstruation, birth control pills) may decrease acidity, favoring the growth of yeast
- Antibiotics kill bacterial populations that produce acid, reducing acidity and favoring yeast growth
- In women, usually yeast infections are an overgrowth of normal flora, but they can be STD's
- In men, 10% are STD's
- Symptoms
- In men, urethritis, red, swollen, itchy glans
- In women, vaginitis, vaginal discharge (white, with curdlike lumps, yeasty odor), itching, redness, painful intercourse
- 20% of all vaginitis is caused by Candida
- Complications and cautions
- Irritation due to yeast infections can increase the chance of secondary bacterial infection
- Infants commonly have oral yeast infections (thrush, also seen in AIDS patients), that can be transferred to the mother's nipples by a nursing infant
- Diagnosis--observation of characteristics of discharge and microscopic observation
- Treatment
- Antifungal creams (Monistat, Lotrimin)
- Formerly vinegar douches, crystal violet dye
- Direct application of live yogurt, to replace acid-producing bacteria
- Well when symptoms are gone, but may be recurrent
- Trichomonas
- Caused by protozoan parasite
- Very common in women
- Often mixed infection with other STD's
- Men are often carriers--asymptomatic (10% may have penile discharge) themselves, but may carry infection to female sexual partners
- Women may have recurrent Trichomonas infections, almost always due to reinfection by a sexual partner, therefore should treat both partners
- Possible (not very likely) to get from warm wet infected environmental contact, like locker room bench, toilet, or infected clothing
- More often transferred by sexual contact
- Incubation period--four weeks
- Location of infection
- In women, vaginitis, cervicitis, urethritis may move to bladder
- In men, urethritis may move to prostate and seminal vesicles
- Symptoms
- In women, heavy foamy yellow-gray foul-smelling vaginal discharge, itching, rash, lower abdominal pain, painful intercourse
- In men, (if any symptoms) white discharge, itching
- Diagnosis: observation of discharge, culture (5 days), microscopic observation
- Treatment
- Flagyl (metronidazole) for seven days
- Should not be given to pregnant or nursing women
- Side effects include nausea and vomitting, headaches, alcohol intolerance
- Must treat both partners ("ping-pongs")
- Cautions for women: can cause changes in cervical cells that cause Pap smear to appear abnormal, should return to normal after treatment, then retest
- Gardnerella (GV)
- Caused by bacteria Gardnerella vaginalis
- Annoying, contagious, but not serious
- Women get GV and have symptoms; men don't have symptoms, but do act as carriers
- If a woman has GV, there is a 50 to 70% chance that her male sexual partner will also have GV
- GV can be normal flora or an STD transferred by sexual contact
- GV "ping-pongs"--must treat both partners
- In women, GV causes vaginitis, formerly called "nonspecific vaginitis"
- In men, GV causes urethritis
- Incubation period: 10 days
- Symptoms in women: light vaginal discharge with fishy odor enhanced by adding KOH to it
- Treatment: antibiotics, for both partners
Reproductive System Cancer--See online handout
- Cancer of the Reproductive System (See online handout)
- Women
- Breast cancer (1/8 to 1/10 chance of diagnosis over entire lifetime, chance increases with age, especially after age 50, when women should begin to get annual mammograms)
- Uterine cancer, cervical (Pap smears) or endometrial
- Ovarian cancer--hard to detect early, so farther advanced and harder to treat at diagnosis
- Men
- Testicular (most common in young men)
- Prostate (older men, PSA test)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}